







Cataracts in Your Eyes? CAUTION on Which Intraocular Replacement Lenses Chosen
Related: astigmatism, clothing and footwear, eyesight, Michael Erlewine, optics, Roy P, sunglasses, Terence M
Michael Erlewine writes (name used with permission):
It has been suggested that I have cataract surgery and receive artificial lenses in my eyes. They also offer these lenses with or without UV protection/coating or whatever.
I worry that how I see color will be affected by the UV coating.
Do you have an opinion about UV coatings or not having that?
DIGLLOYD: as to color perception, the lenses in our human eyes steadily yellow with age, so it is probably inevitable that color perception will change, from that alone.
Far more important would be discomfort causes by highly variable UV/blue transmission which could lead to degenerative issues, as well as color perception caused by too-strong filtering. Try to obtain a spectral transmission chart, and study the available research before making a decision as this field may be changing—recently I saw news on a lens enabling near/far focus unlike previous lenses.
Violet and blue light blocking intraocular lenses: photoprotection versus photoreception
Action spectra for most retinal photosensitisers increase or peak in the violet part of the spectrum. Melanopsin, melatonin suppression, and rhodopsin sensitivities are all maximal in the blue part of the spectrum. Scotopic sensitivity and circadian photoentrainment decline with ageing. UV blocking IOLs provide older adults with the best possible rhodopsin and melanopsin sensitivity. Blue and violet blocking IOLs provide less photoprotection than middle aged crystalline lenses, which do not prevent age related macular degeneration (AMD). Thus, pseudophakes should wear sunglasses in bright environments if the unproved phototoxicity‐AMD hypothesis is valid.
DIGLLOYD: sounds like (speculating here) it is a bad idea to block blue, because it would affect circadian rhythms and hormones.
Terence M writes:
One of the best surgeons in the world is Dr. Raymond Stein in Toronto. www.bochner.com
My friend was a Captain on the B737 at WestJet (Similar to Southwest), he lost his aviation medical for some sort of eye problem and after several laser surgeries a doctor recommended he see Raymond Stein, apparently he was the only eye doctor could fix the problem. He did and he returned to work. Also a lot of Americans go there for treatment. My optometrist said he is world famous, wrote books on the topic and teaches at the University of Toronto. Though, such a hassle now to cross the boarder with COVID.
DIGLLOYD: good to know.
Alek O writes:
FYI FWIW that here is my (War & Peace!) writeup about my experience with Cataract Surgery. Here's my sub-page that talks about spectral transmittance ... and yes, you can see Ultraviolet after Cataract surgery! ;-)
I get about an Email a month from random people basically "thanking" me for that webpage since it explains what they "see" ... although you hardly notice in day-to-day ... just mostly around stuff like UV lights. Note this is different than how the world looks "whiter" after Cataract Surgery that removes the yellowing natural lens.
I personally LOVE seeing the deep purple/violets of sunrise/sunsets ... so if that is something you like to see, be careful getting a blue-blocker IOL. alek
P.S. You comment about IOL's that enable near/far focus ... I assume you are referring to multi-focals. Those have been around for a decade plus ... and sure, the newer "extended depth of focus", etc. are better. Be careful there also - the laws of (optical) physics apply.
...(later)...
So yea, I think some concerns that the Crystalens in my eyes are too transmissive below 400nm ... so I am very good about wearing sunglasses when out. However, the question is where do you draw that line ... because with blue blockers, you'll filter out some of the visible ... so are you willing to give up those deep purple/violets of sunrise/sunsets?
Dr. Mainster (discussed/linked on my web page ... who I actually chatted with a while back) doesn't seem to be a fan of blue blockers. And while I haven't looked much in recent literature, here's a 2018 survey paper that concludes: "Based upon current, best-available research evidence, it is unclear whether blue-light filtering IOLs preserve macular health or alter risks associated with the development and progression of AMD, or both."
BTW, I would not be surprised that many older patients who have blue blocker IOL's implanted actually DO end up seeing BETTER in the blue/purple regime ... just because their natural lens was filtering so much of that light. However, if the IOL is BLUE-blocking, then by definition, they aren't seeing the colors they saw when they were younger.
Finally, I should mention (and add to my website) a very recent NEW addition in the IOL field which is the Light Adjustable Lens which JUST got approved. This is pretty cool as they can adjust the power (spherical and cylinder) AFTER the IOL is implanted ... so you can really "dial it in" ... and adjust post-op for any misses. It does this via (surprise!) UV ... so you, of course, have to ALWAYS were UV glasses during the adjustment phase before you "lock" it in - read more here.
P.S. Some of the links on my web pages have unfortunately broken over time. I did update the link about Monet's paintings were affected by his cataract and then removal which is a nifty story if you haven't read it before - there's a link there to a PDF version has the images embedded.
DIGLLOYD: great info at the links above!
I spend a lot of time at very high altitude (10K to 12K feet), where there is far more UV and blue/violet up there. My contact lenses block UV and so do my sunglasses, but skin burns come on quick without sunblock and I can't always wear sunglasses (and don’t early and late in the day).
Another concern is light sensitivity at a computer screen—my father has that and he has has IOL's in both eyes. Dunno if the sensitivity is blue light or not—maybe something else.
Roy P writes:
Re. cataract surgery, I had both eyes done just about ten years ago, and I had put together the images below to explain to people how my vision improved before and after the surgery, and my natural eye lenses got swapped for intraocular replacement lenses.
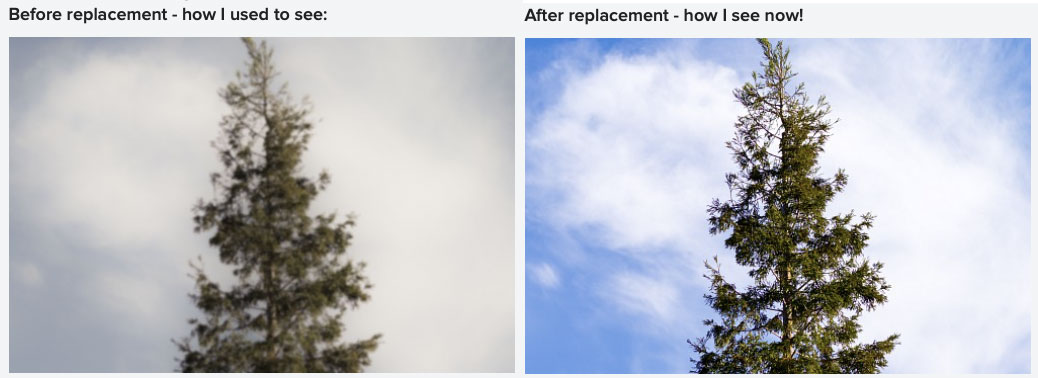 Perceived clarity before/after cataract surgery (Roy P)
Perceived clarity before/after cataract surgery (Roy P)Even then, there were a whole bunch of options offered, including lenses corrected for astigmatism, distant vision, even reading, etc.
The problem is, an implant being placed in the eye ball is not like a lens being mounted on a camera with a fixed and rigid mount. By the time lens settles down in the eye over several months, even a couple of years, it goes through slight changes to its placement in all three dimensions.
So whatever correction was built into the lens would no longer be valid, and you’d have to get corrective lenses to compensate for undoing the settlement changes, and that is never perfect. And if you’re going to be wearing glasses anyway, why complicate the implants?
So I just got two very basic lenses that give me 20-20 vision from a distance of about 3 feet to about 20 feet, and that is good enough that I can drive without wearing any glasses in known places where I don’t need to precisely read street signs or names. I do wear progressives that have distant vision built into them at the top and a reading prescription at the bottom. But in between, my glasses are largely without any power, except for slight correction for some astigmatism.
After my surgery in 2010, I’ve had four eyeglass prescriptions. The first was shortly after the surgery, the second was a year later, the third was another year later. The fourth was about five years ago. Since then, there is a very slight change, as of my most recent eye test about a month ago, but it is so negligible that a new pair of eyeglasses was not warranted.
Over the years, I have been advising the same strategy to others
I also got a pair of +4 prescription reading glasses for being able to see the LCD back of the camera on a tripod for Live View focusing. So I take off my regular glasses and put these on when I need to look at the LCD closely. I did get UV protection in my implants. So I only wear sunglasses for comfort
So that’s one data point to consider for anyone planning to get cataract surgery done.
DIGLLOYD: great advice. I think for now such a surgery would drive me crazy—I’m going to stick with my contact lenses as long as I can. I don't have clarity issues, only correction and things are pretty stable.
Ultraviolet or blue-filtering intraocular lenses: what is the evidence?
Jan 8 2016
Abstract
Cataract surgery was revolutionised by the introduction of modern intraocular lenses in the late 1940's. By the late 1960's to 1970's evidence had emerged that short-wavelength light caused phototoxicity at the retina and retinal pigment epithelium. By the early 1980's ultraviolet filters had been incorporated into intraocular lenses. This caused intense controversy, as there was concern that the UV-filtering chromophore might leach out into the eye causing toxicity. With the arrival of blue-filtering intraocular lenses (BFIOLs) in 1990's, a further debate was ignited as to their safety and potential disadvantages.
Selecting the optimal performing intraocular lens to obtain the best visual performance with the fewest potential drawbacks has become complex and challenging for cataract surgeons and their patients with the wide choice of lenses available. Choosing a personalised lens to address astigmatism, presbyopia, spherical aberration, chromatic aberration, and potentially to shield the retina from short-wavelength light is now possible.
The potential benefits and possible side effects of these different innovations emphasise the importance of assessing the evidence for their clinical utility, allowing the surgeon and the patient to weigh-up the risk benefit ratio and make an informed decision. The BFIOLs were developed to reduce cyanopsia, address chromatic aberration, and improve contrast sensitivity in different lighting conditions, as well as to prevent short-wavelength light reaching the retina thus potentially reducing the risk of developing age-related macular degeneration. Further design development of the BFIOLs was to mimic the natural crystalline lens absorption and transmittance properties in adulthood.
Multiple publications have reported on the potential benefits and pitfalls of implanting a blue-filtering lens. The potential disadvantages raised in the literature over the last 25 years since their introduction, regarding compromise of visual function and disruption of the circadian system, have been largely dispelled. The clear benefits of protecting the retina from short-wavelength light make a BFIOLs a sensible choice. The purpose of this article presented at the Cambridge symposium 2015 is to review the literature on this subject...
Discussion
...Overall, it would seem that there are no drawbacks to using a BFIOL, and indeed there are benefits of using an IOL which filters out short-wavelength light including reduction in glare.11, 48, 49, 50 However, more importantly as short-wavelength light has been shown to be toxic to the retina and results of in vitro, animal and clinical studies support the hypothesis that protecting the retina from short-wavelength light is desirable, implantation with a BFIOL seems a sensible precaution...
...There are a wide range of IOLs available and it is not within the scope of this article to specifically discuss any particular IOL. However, it is important that the IOL design allows photoreception as close as possible to the young adult healthy crystalline lens, and photoprotection to prevent short-wavelength light damage over the lifetime of the recipient.
DIGLLOYD: choices are far better here in 2021 than a decade ago.
